MITE PSQI Hot Topic- March 2020: Failure Mode(s) and Effects Analysis (FMEA)
Erin Graydon Baker, MS, RRT, CPPS, CPHRM
Clinical Risk Manager, MaineHealth
Learning Objectives:
- Recognize the differences between Root Cause Analysis and Failure Mode(s) and Effects Analysis (FMEA)
- Describe the application of FMEA techniques to any new or existing process
Failure Mode(s) and Effects Analysis (FMEA) versus Root Cause Analysis (RCA):
What’s the difference and which investigative, quality improvement method should I choose when evaluating harm or potential for harm? FMEA is a proactive risk assessment, whereas RCA is a reactive risk assessment.
RCA:
- A thorough and credible case review to identify basic or contributing factors underlying variation in performance
- Focus is on processes, systems, and culture, not on individual performance
- Focus relates to a specific case that either caused harm or had the potential to cause harm
- Thorough and credible is defined as multidisciplinary participation and inclusion of subject matter experts, facilitated by trained individuals.
- Uses Tools including time lines ( sequence of events) , fishbone diagram, action plans
FMEA:
- A systematic method of identifying and preventing process failures before they occur
- First formal FMEAs were conducted in aerospace industry to look for safety issues
- FMEA was used primarily to look at new processes to identify points of failure before launching a new process or product but is also used to review existing processes
- RCAs focus on how did particular adverse event occur whereas FMEAs focus on how could an adverse event occur
- RCAs can guide an FMEA; using specific cases to highlight system weaknesses
- FMEA similarly to RCA, uses tools to help evaluate potential failures
- FMEA starts with a flow/process map
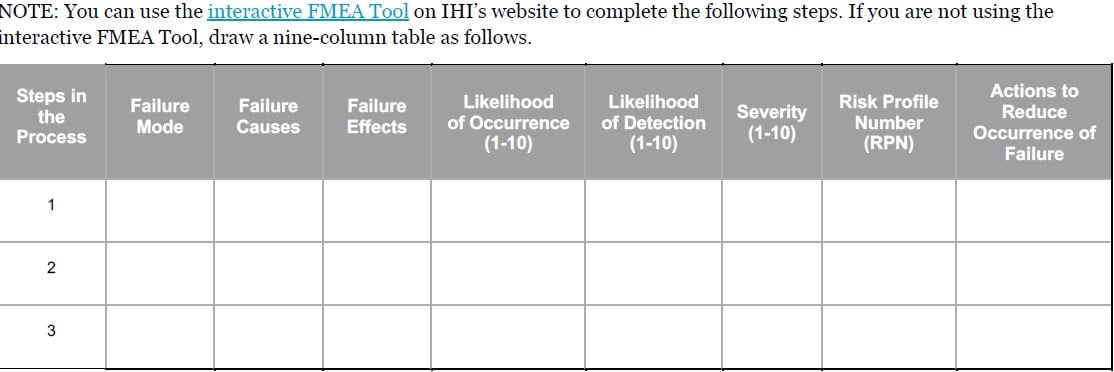
FMEA brings subject matter experts, both optimists and pessimists, in a room together to review each step in a new or existing process. Typically, the facilitator(s) prepares a process map in advance of the exercise. Tracking through the process steps, the group discusses potential failures, the likelihood that certain failures will occur and the potential for harm to a patient or to operations if a failure occurs. The likelihood (probability) and the potential for harm (severity) are each scored and then multiplied to assign a risk priority number, or RPN. The RPN helps the team prioritize which are the most vulnerable steps to fix.
This process can become more sophisticated by adding another variable such as ability to detect the failure before it happens. If we have alarms that warn us or electronic hard stops to prevent an error, we can decide that a particular step is safe and needs no intervention.
Once the high RPN step failures have been prioritized, the team assigns responsible persons to complete the corrective action items that will mitigate the chance of each failure occurring. Each responsible person will provide updates to the team and ask for help in removing barriers.
Once the FMEA action items are completed, the team measures the success and modifies the process as appropriate in PDSA (Plan-Do-Study-Act) format.
Here’s the sample template used to list the steps, failures, RPN scoring and action planning.
Anyone can do this process using this format. You must be sure that you have appropriate leaders who can help remove barriers engaged from the beginning of the process.
For more information; use the link provided or contact:
Download PDF