How to teach Operational Excellence Techniques during clinical precepting
Elizabeth Eisenhardt, MD, FACP
Operational Excellence and Quality Improvement principles can provide ripe educational opportunities beyond the standard format of lectures or book reading. Quality Improvement/Operational Excellence principles can be taught “in the moment”, “at the bedside” or “just in time” during clinical precepting sessions. In the following article, I will give you some examples of how to achieve this.
To begin, let’s review the definitions of Quality, Improvement, and Operational Excellence. Quality can be defined as “The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge AND the degree health services meet the expectations of healthcare users (the marketplace).” In the words of the famous scholar Juran, he describes quality as the following:
- Attaining professionally agreed standards of care.
- Something that is good, serves the purpose,
and is worth the money that is paid for it - Reducing the variation around the target.
Improvement can be defined as “A change for the better (Kaizen), and not simply a change, but one which is supported by data, not a judgement call. “ Quality Improvement work tends to be proactive, continuous process improvement work to shift a culture or to exceed expectations.
Operational Excellence can be described as a philosophy that embraces problem-solving and leadership as the key to continuous improvement with the change ideas coming from the “real place of work” or Gemba.
One of the founding principles of Operational Excellence is the 8 types of waste as pictured in the waste wheel pictured below:
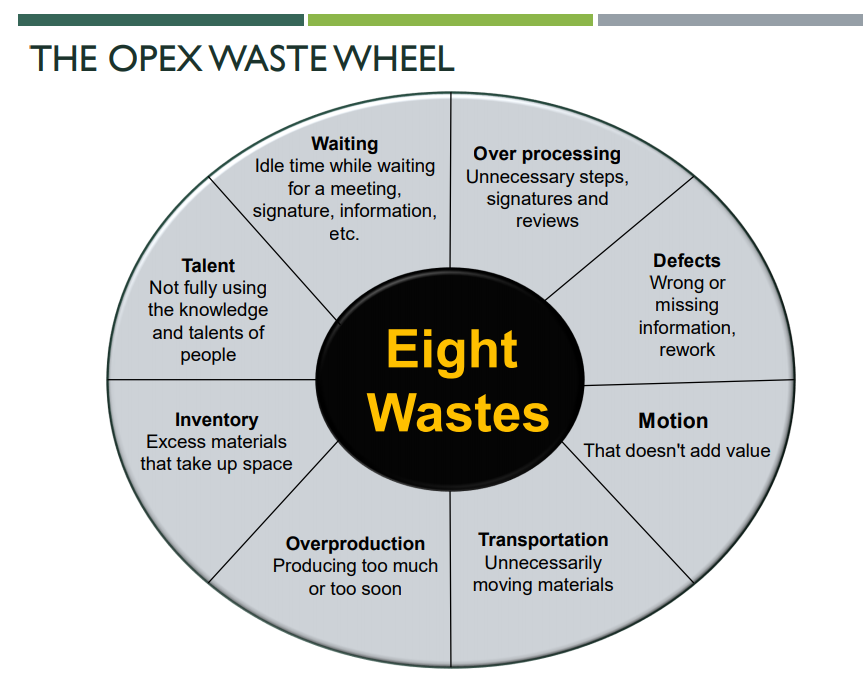
If you keep a copy of this wheel close by while precepting, it can be useful to pull it out and ask a learner to identify a type of waste they observed during a certain patient interaction. Perhaps the learner is running late, because the patient had excess WAITING time to be roomed, or to check-in, or to enter the building after being asked screening questions. Perhaps they observed TRANSPORTATION waste if a certain medication or vaccine is kept only on one floor and the staff had to retrieve it. There are numerous examples of waste that can be observed and discussed.
Another quick way to keep Operational Excellence alive in the moment of clinical precepting is to ask a learner to come up with a KPI ( Key Performance Indicator) that could be applied to their patient to achieve a missing quality metric. For example, if they are telling you how their diabetic patient is missing their A1C (measurement of their blood sugar), you can pause and ask the learner, “Can you think of a KPI that might help you capture more A1C ‘s on your patients?” The answer may be something along the lines of “100% of diabetic patients will schedule a one month follow-up at time of check-out” or “100% of diabetic patients seen in the office due for A1C will have this test ordered at time of visit.” KPIs can be applied to nearly any quality metric to help improve results. KPIs are then posted to the clinical sites’ KPI board and seen during Operational Excellence Gemba board walks.
Helping learners to develop their Quality Improvement skills can have multiple benefits for them including increased engagement, increased understanding of the “bigger picture” and increased appreciation for inter-professional teamwork. I hope you will try out some of the techniques above!
References:
Website for the Institute for Healthcare Improvement: Improving Health and Health Care Worldwide | IHI – Institute for Healthcare Improvement
MMC Canvas: Quality Improvement Science Guide: Quality Improvement Science Guide (instructure.com)
Want to earn CE credits? Click here
Download PDF