March 2021 MITE Quality Improvement Patient Safety Hot Topic
Avoiding the “Whack-a Mole” Approach to Patient Safety Events: the Safety Assessment Code matrix
Erin Graydon Baker, MS, RRT, CPPS, CPHRM
Clinical Risk Manager, MaineHealth
Learning Objectives:
- Describe how and when to prioritize immediate safety threats
- Explain the Safety Assessment Code ( SAC) matrix
In the December 2020 MITE Hot Topic, “Prioritization Methods: Which QI Project Solution Ideas Should We Tackle First?” author Lauren Atkinson describes the impact to effort matrix for quality improvement. The impact to effort matrix helps us to prioritize the most impactful improvements and discriminates them from efforts which may be too great for the anticipated impact. A prioritization process for safety that is described by the Institute for Healthcare Improvement (IHI)/ National Patient Safety Foundation (NPSF) is similar in intent but more applicable to identifying and classifying adverse events and near misses.
All healthcare personnel are encouraged to report hazards, near misses, and adverse events that reach the patient regardless of whether injury occurs to the patient or staff. Failure to report can negatively affect our ability to mitigate the risk of harm. Solutions to ensuring staff reporting include an easy to use on-line reporting system, visible actions as the result of reports, and feedback to staff when the reports have led to improvements. For some personnel, though, the reports seem to disappear into the “black hole” of reporting systems where seemingly nothing is done with the information. To those receiving the safety reports, the daily work of reviewing and acting upon the all reports seems like a poor game of “Whack-a Mole” – when one issue seems resolved, another similar event pops up somewhere else. It can be both exhausting and non-productive to react to each event. How should we prioritize the most significant events while trending and tracking those events that may be latent errors leading to something harmful?
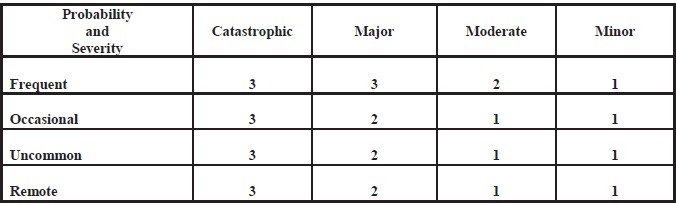
The IHI/ NPSF describes a process called the Safety Assessment Code (SAC) matrix. SAC multiplies the probability that another event will happen if nothing is done by the actual and/or potential harm to patients or staff to assign a severity score. The highest scores deserve a deeper level of investigation whereas a lower score indicates events that should be trended and tracked over time. This level of prioritization allows for targeted improvements where it will matter most without losing sight of those latent errors that provide valuable information over time.
The matrix below describes how to score severity and probability in order to assign an overall safety score. To use this grid, estimate how frequently this same event might occur. For example, falls might occur frequently, but historically, the actual or potential harm has been low because of the interventions we have in place to reduce serious harm. A frequent event with minor harm would score “1” and would signal us to trend these. However, if we had a 10-fold medication error in dosage which, although uncommon, could have a catastrophic impact on the patient, then the score would be “3”. This would warrant a full Root Cause Analysis.
A trained safety team uses this method best with interrater reliability in scoring and prioritizing events. Understanding SAC helps those who file reports recognize that all reports are reviewed with triage in mind. Some will receive intensive review, while others will contribute to data aggregation and monitoring.
For more details on the probability and severity categories, use the link (1): http://www.ihi.org/resources/Pages/Tools/RCA2-Improving-Root-Cause-Analyses-and-Actions-to-Prevent-Harm.aspx
References
- National Patient Safety Foundation. RCA2: Improving Root Cause Analyses and Actions to Prevent Harm. Boston, MA: National Patient Safety Foundation; 2015.
Want to earn CE credits? Go to CloudCME to review the materials, take a short quiz and evaluation!
Download PDF